Reviewed by: Shoaib Abid
CEO, Revenue Cycle Management & Provider Credentialing Specialist
Last Reviewed: July 2026
If your practice bills Medicare Advantage, Medicaid managed care, CHIP, or a Qualified Health Plan on the Federal Exchange, the rules for prior authorization changed on January 1, 2026. The decision windows got shorter. Denials now require a specific reason. And in six states, Original Medicare started requiring prior auth for the first time in decades.
You’ve probably already felt the impact. Practices that don’t adapt their workflows risk delayed approvals, increased claim denials, and slower reimbursements. Strengthening your insurance verification process and implementing proactive denial management services can significantly reduce authorization-related revenue loss. This guide explains exactly what changed under the 2026 CMS rules, how to update your billing workflow, and where most practices are losing revenue because they haven’t caught up yet. For a deeper look at the latest CMS updates, read our guide on Prior Authorization Medical Billing: 2026 CMS Rules.
What changed on January 1, 2026
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) went into operational effect on January 1, 2026. Three things changed at once.
Standard prior authorization decisions now have a 7 calendar day limit. Before this rule, many payers took up to 14 days. That window is cut in half. According to CMS, this represents a 50 percent improvement for some payers.
Expedited (urgent) decisions must come within 72 hours. Same rule, tighter window for cases where the standard timeline could jeopardize a patient’s health.
Denials now require a specific reason. Payers can no longer hand you a generic denial. They must tell you exactly why the request was denied, regardless of whether they communicate it by portal, fax, email, mail, or phone. This makes the appeals process much more effective and allows providers using denial management services to identify denial trends, submit stronger appeals, and recover reimbursement faster.
These requirements apply to Medicare Advantage organizations, state Medicaid and CHIP Fee-for-Service programs, Medicaid managed care plans, CHIP managed care entities, and QHP issuers on the Federally-Facilitated Exchanges. Drugs are excluded from this rule. They’re governed separately under the proposed CMS-0062-P rule, which is open for public comment through June 15, 2026.
One quick note on the API side. The rule also requires payers to stand up four FHIR APIs (Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization), but those compliance dates got pushed from January 2026 to January 2027. So the electronic prior authorization infrastructure you’re hearing about is coming, just not live yet for most payers.
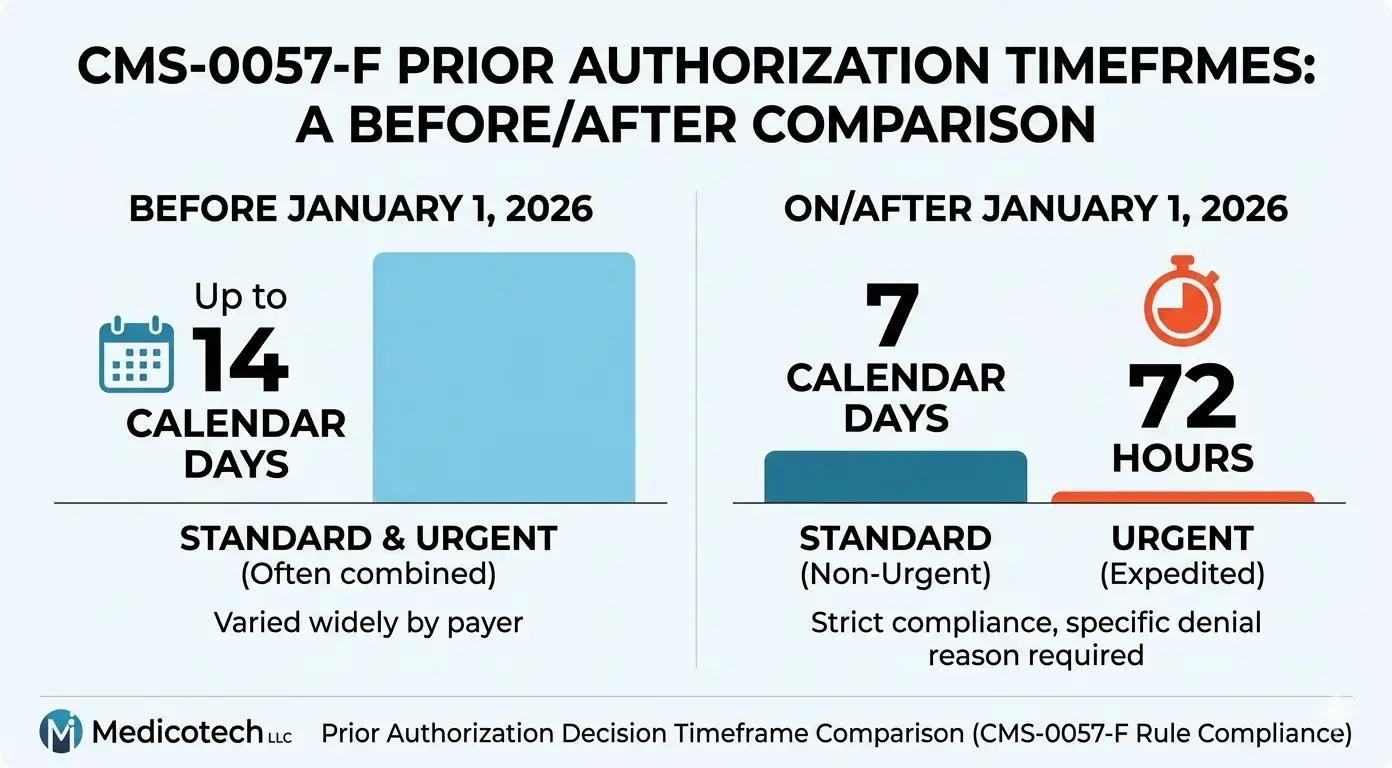
The new decision timeframes at a glance
| Request type | Old timeframe | New timeframe (Jan 1, 2026) |
| Standard (non-urgent) | Up to 14 calendar days | 7 calendar days |
| Expedited (urgent) | Varied by payer | 72 hours |
| Drug prior authorization | Not covered by this rule | Proposed under CMS-0062-P |
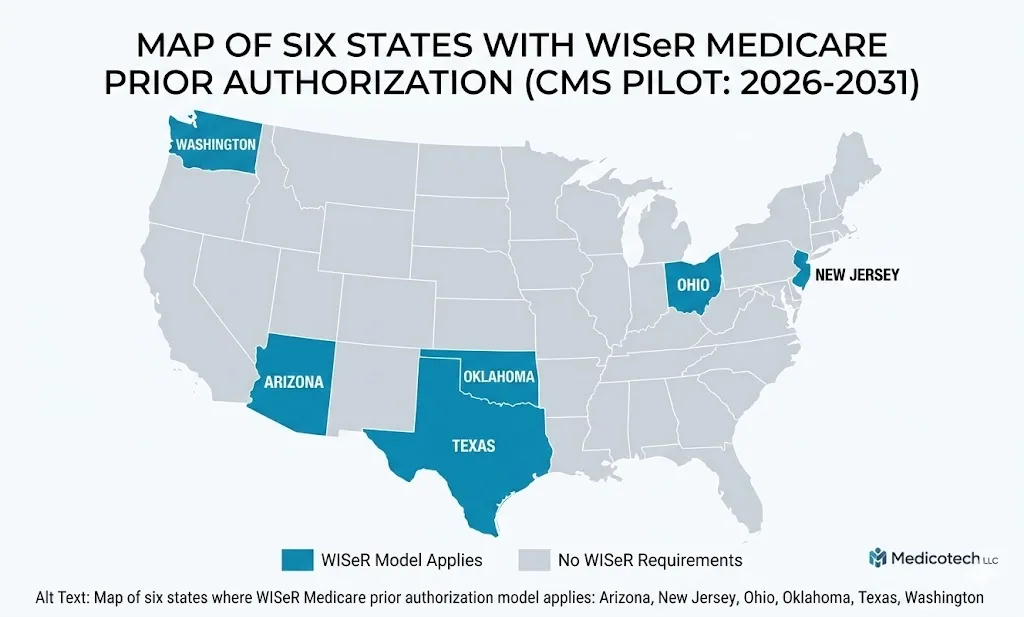
What WISeR Medicare means for practices in 6 states
If you bill Original Medicare in Arizona, New Jersey, Ohio, Oklahoma, Texas, or Washington, there’s a second change you need to know about. CMS launched the Wasteful and Inappropriate Service Reduction (WISeR) Model on January 1, 2026, with prior authorization requests starting January 5 and services beginning January 15.
This is a 6 year pilot running through December 31, 2031. It’s the first time Original Medicare (not Medicare Advantage) has required prior authorization for outpatient services in most of these categories.
WISeR applies to a specific list of services, including:
- Percutaneous image-guided lumbar decompression for spinal stenosis
- Arthroscopic lavage and debridement for osteoarthritic knee
- Epidural steroid injections for pain management (excluding facet-joint injections)
- Percutaneous vertebral augmentation for compression fractures
- Cervical fusion
- Nerve stimulator implants
- Skin substitutes for chronic wounds
- Impotence treatments and incontinence devices
Coverage decisions are expected within 72 hours (48 hours for expedited). Once approved, the authorization is valid for 120 calendar days. Denied requests can be resubmitted with additional information, and you can request peer-to-peer clinical review. There’s no limit on resubmissions.
Participation is technically voluntary. But if you don’t submit prior authorization, your claims go through post-service pre-payment medical review instead, which can significantly delay reimbursement and disrupt cash flow. For most practices in the six participating states, requesting prior authorization is the faster path. Many healthcare organizations also rely on revenue cycle management services to streamline prior authorization workflows, reduce payment delays, and maintain consistent reimbursement.
One practical detail: Medicare Advantage patients are not affected by WISeR. This is Original Medicare only. If your patient panel skews Medicare Advantage, your exposure is limited. If it skews traditional Medicare, your billing team needs a WISeR playbook by service line.
Does Your Practice Lose More Than 10% of Its Revenue to PA Denials?
You don’t have to guess—book a free 30-minute billing audit today. We’ll review your last 90 days of submissions and show you exactly where your revenue is leaking.
Why prior authorization breaks your revenue cycle
Here’s the honest part most billing companies won’t say out loud. Prior authorization is the single most underrated driver of denied claims in a typical practice. The AMA has documented that physicians spend roughly 15 hours a week per provider just on PA paperwork. Akasa’s research found that a single PA submission and status check takes 12 minutes and 7 seconds on average. Multiply that by the 41 PAs the average physician handles weekly, and you see where the revenue leak starts.
The top 5 places your revenue gets stuck:
- Missing prior authorization submitted after service. The service was performed, the documentation is fine, but no one got auth first. Denial. Retro auth sometimes works, often doesn’t.
- Incomplete clinical documentation in the PA request. Payer asks for additional records. Clock stops. Clock restarts. Seven days becomes fourteen.
- Wrong CPT or HCPCS code in the request. Auth gets approved for the wrong code. Claim submitted with the actual code. Denial for no authorization on file.
- Authorization expired before service was performed. Most auths have windows. Miss the window, restart the process.
- Peer-to-peer review not requested. When a request is denied, many practices give up. You can almost always escalate to a physician-to-physician review that reverses the initial determination.
At 500 claims per month averaging $150 per claim, a 15% prior authorization denial rate costs your practice roughly $11,250 per month in delayed or lost revenue. Most of it is recoverable, but many practices fail to appeal or correct these claims. Learning how to reduce medical claim denials in 2026 can help minimize authorization-related denials and improve your overall reimbursement rate.
How to adapt your billing workflow to the new 2026 rules
This is the section practice managers actually need. Five concrete workflow changes that close the revenue leak under the new rules.
1. Reset your payer tracking to 7 day standard decisions
If your team is still building their follow up schedule around the old 14 calendar day window, they’re calling too late. Pending requests should be flagged for review at day 4
escalated at day 6, and reported as overdue at day 8. For expedited requests, flag at hour 24, escalate at hour 48, overdue at hour 72.
Build this into your practice management system as a rule, not a memory test. Staff turnover in billing is high. A biller who joined last month won’t remember the old 14 calendar day window, but they also won’t catch a pending auth that’s sliding past day 7 unless the system tells them to.
2. Use the specific denial reason requirement to rebuild your appeals playbook
Before January 2026, a lot of denials came back with vague language. “Not medically necessary.” No detail. Hard to appeal. Under the new rule, the payer must tell you the specific reason.
Use that. Build a denial reason library by payer. When you see the same specific reason three times from the same payer, that’s a workflow gap, not an appeals problem. Fix the gap upstream. The appeal is the symptom.
3. Scrub prior auth requests against payer rules before submission
Most denials stem from easily avoidable errors: wrong code, missing documentation, eligibility gaps, or missing signatures. Build a pre-submission scrub step that checks every request against the specific payer’s documented requirements before submission. Combining this process with health insurance verification services helps confirm patient eligibility, benefits, and authorization requirements before treatment, significantly reducing preventable denials.
We see practices running 22 percent PA denial rates drop to under 8 percent within 90 days of implementing scrubbing. The denials you prevent are worth far more than the ones you win on appeal.
4. For WISeR states, assign a dedicated specialist
If your practice operates in Arizona, New Jersey, Ohio, Oklahoma, Texas, or Washington, and you bill Original Medicare for any of the WISeR service categories, don’t make this a shared responsibility. One person should own it. They need to know the state’s assigned WISeR participant (Zyter TruCare in Arizona, Virtix Health in Washington, and different participants by MAC jurisdiction), the 120 calendar day validity window, and the peer to peer escalation process.
Spread this across 4 billers and every biller owns a part and no biller owns the outcome.
5. Plan for the API transition coming January 2027
The electronic prior authorization infrastructure goes live for most payers on January 1, 2027. Your EHR and billing system vendors are building toward that date now. Ask your vendor directly: will you support FHIR-based Prior Authorization API submission by Q4 2026? If the answer is vague or “we’re looking into it,” that’s a red flag for where your workflow will be in 12 months.
Practices that adopt early will see decision times drop from days to hours on compatible payers. Practices that wait will fall further behind.
Ready to Stabilize Your Cash Flow in 2026?
Closing these workflow gaps is the fastest way to protect your revenue. If you’re ready to offload the burden of these new rules, schedule a consultation with our RCM team today to see how we handle PA throughput at scale.
Medicotech’s approach to prior authorization in 2026
Here’s how we handle it for the practices we bill for. This is the operational side, not marketing language.
Every PA request goes through pre submission eligibility verification against the specific payer’s current documented requirements. A dedicated specialist per client tracks pending requests on a 7 calendar day standard and 72 hour expedited cadence. Denials get routed the same day to appeals triage. Peer to peer reviews are requested within 48 hours of denial when clinically warranted. WISeR state practices get a separate playbook built around the 120 calendar day validity window and MAC jurisdiction specific participants.
The proof metric we track is first pass PA approval rate. Industry baseline sits around 75 percent. Our target is 92 percent or higher within 90 days of onboarding a practice. That single metric determines whether your cash cycle tightens or loosens over the next year.
Frequently asked questions
What is the new CMS prior authorization rule for 2026?
CMS-0057-F requires impacted payers to decide standard prior authorization requests within 7 calendar days and expedited requests within 72 hours, starting January 1, 2026. Payers must also provide a specific reason for any denial. The rule applies to Medicare Advantage, state Medicaid FFS, CHIP FFS, Medicaid and CHIP managed care plans, and QHP issuers on the Federal Exchanges. It does not apply to drug prior authorizations.
How long does prior authorization take in 2026?
Standard requests must receive a decision within 7 calendar days. Expedited (urgent) requests must receive a decision within 72 hours. These timeframes apply regardless of how the request is submitted, so payers cannot claim slower timelines for faxed versus electronic requests.
What is WISeR Medicare?
WISeR (Wasteful and Inappropriate Service Reduction) is a CMS pilot that introduces prior authorization requirements in Original Medicare for select outpatient services. It runs from January 1, 2026 through December 31, 2031 in six states: Arizona, New Jersey, Ohio, Oklahoma, Texas, and Washington. It does not affect Medicare Advantage enrollees.
Which services does WISeR apply to?
WISeR currently covers about 17 service categories, including epidural steroid injections, knee arthroscopy for osteoarthritis, cervical fusion, percutaneous vertebral augmentation, nerve stimulator implants, skin substitutes for chronic wounds, and incontinence and impotence devices. The full list with HCPCS and CPT codes is in the WISeR Operational Guide published by CMS.
What happens when prior authorization is denied?
Under the 2026 rule, the payer must provide a specific reason for the denial. You can resubmit the request with additional clinical documentation, request a peer-to-peer clinical review between the requesting physician and a payer medical reviewer, or file a formal appeal depending on the payer’s process. There is no limit on the number of resubmissions for WISeR requests.
How do I appeal a prior authorization denial?
Start by reviewing the specific denial reason the payer is now required to provide. If the reason is about missing documentation, gather the records and resubmit. If it’s medical necessity, request a peer-to-peer review before filing a formal appeal. Formal appeals follow the payer’s published process with specific deadlines that vary by plan type.
Do Medicare Advantage plans still require prior authorization in 2026?
Yes. Medicare Advantage plans require prior authorization for many services and are now subject to the same 7 calendar day standard and 72 hour expedited decision timeframes under CMS-0057-F. They must also provide specific denial reasons starting January 2026.
What is electronic prior authorization?
Electronic prior authorization (ePA) uses standardized APIs to let providers check authorization requirements, submit requests, and receive decisions digitally rather than by fax or phone. Under CMS-0057-F, impacted payers must implement a Prior Authorization FHIR API by January 1, 2027. Some payers already offer ePA through existing clearinghouses.
How does the denial reason requirement help with appeals?
Before 2026, denials often arrived with vague language like “not medically necessary” without detail. Under the new rule, payers must explain exactly why the request was denied. This lets billing teams identify patterns, fix upstream workflow issues, and build targeted appeals rather than guessing what the payer wanted.
What’s the difference between prior authorization and pre certification?
They’re used interchangeably in practice, but technically pre certification often refers to verifying that a service will be covered before it’s rendered, while prior authorization specifically requires the payer’s approval before the service is provided. The 2026 CMS rule governs prior authorization decisions.
Does the new CMS rule apply to commercial insurance?
CMS-0057-F directly applies to Medicare Advantage, Medicaid and CHIP (FFS and managed care), and QHPs on the Federally-Facilitated Exchanges. Commercial plans not in these categories are not directly regulated by this rule, though many are adopting similar standards voluntarily. State level laws also govern commercial plan prior authorization in many states.
How can outsourcing help with prior authorization?
A dedicated PA specialist knows each payer’s current documentation requirements, tracks the new 7 calendar day standard and 72 hour expedited windows, and escalates peer to peer reviews quickly. For most small and mid size practices, this work is done by a biller juggling 12 other responsibilities. That’s where the revenue leak starts. Outsourcing moves it to someone whose only job is PA throughput.
What happens if my practice misses the 7 day window?
The 7 day window is on the payer, not you. If the payer fails to respond within 7 calendar days for a standard request or 72 hours for expedited, that’s a compliance issue you can escalate through the payer’s grievance process or through CMS’s public reporting mechanism. Payers must publicly report their PA metrics annually starting March 31, 2026.
Stop losing revenue to prior authorization denials
Prior authorization is not a paperwork problem. It’s a revenue problem disguised as a paperwork problem. The practices that adapted their workflows to the January 2026 rules are capturing money the practices that didn’t are leaving on the table.
If your PA denial rate is above 10 percent, or your team is still working on a 14 calendar day standard response window, or you haven’t built a WISeR playbook and you bill Original Medicare in one of the six pilot states, you have a fixable problem.
Book a free 30 minute billing audit. A dedicated specialist reviews your last 90 days of PA submissions, identifies the workflow gaps costing you revenue, and shows you exactly where the leak is. No commitment. No setup fees. You get the findings whether you engage us or not.